What is RSI?>> RSI muscle triggers>> RSI nerve triggers>> RSI pathophysiology>> RSI treatment >>Musicians>>Myths>>Inspiration
What is RSI?
RSI is a general term used to describe a primary cause of a condition. It can also indicate an aggravating factor of a pre-existing condition. It simply refers to the repeated use of particular muscle groups as causative and/or aggravating factors.
Most often it is used to classify conditions related to computer work. It also includes most commonly wiriting with pen/pencil, activities involving prolonged periods of gripping, playing musical instruments, typing and mousing.

WRULD or Work Related Upper Limb Disorders is a term coined by the TUC (the British Trades Union Council) meaning repetitive strain induced by one's employment. This term includes conditions such as 'beat hand', 'white finger syndrome' and various other work related syndromes.
 The principle is simple. For example if I were to stroke my cats' chin with my index finger once, there would be no problem, but if I were to do this one thousand times in an hour, both my index finger tendons and my cat would complain bitterly. The muscles and tendons effecting the movement would become tired and begin to ache. They should recover soon. But if I were then to perform the same activity each day for a week, I would probably find that I could only repeat it a few times before my muscles would feel tired and achey, plus, my cat, now with a bald chin would not be pleased.
The principle is simple. For example if I were to stroke my cats' chin with my index finger once, there would be no problem, but if I were to do this one thousand times in an hour, both my index finger tendons and my cat would complain bitterly. The muscles and tendons effecting the movement would become tired and begin to ache. They should recover soon. But if I were then to perform the same activity each day for a week, I would probably find that I could only repeat it a few times before my muscles would feel tired and achey, plus, my cat, now with a bald chin would not be pleased.
Thus, any action repeated too many times, no matter how light, will produce a repetitive strain. 'Nintendo and Blackberry thumb' are classic examples.
RSI trigger areas: musculo-skeletal
What is RSI?>> RSI muscle triggers>> RSI nerve triggers>> RSI pathophysiology>> RSI treatment >>Musicians>>Myths>>Inspiration
Why do some people get RSI from a particular activity whilst others performing the same activity are seemingly immune?From my observations it would appear that the main factors in giving an increased likelihood for RSI fall into the following categories:
- Musculo-skeletal.
- Neural encroachment and compression.
- Degree of time spent performing activities.
- Intensity of actions required
Musculo-skeletal factors consist of the shortening and tightening of any or all of the following trigger areas:
- Lower Cervical deep spinal muscles and Osteopathic lesions in this area
- Upper ribcage lesions, most commonly where ribs 1 to 3 are stuck in an elevated position. This commonly exists along with deep tension in the upper fibres of Trapezius, the intercostal muscles and spinal muscles overlying the upper dorsal spine
- Tension patterns in the rotator cuff muscles, principally Teres major and minor, Infraspinatus, Subscapularis, Supraspinatus and Pectoralis Minor
- The deep fibres of Biceps with occasional involvement of Brachialis
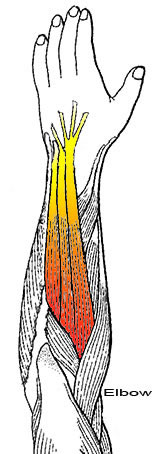
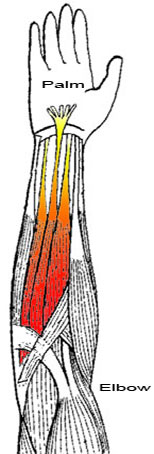
- The superficial and deep flexors of the wrist and fingers and thumb which lie on the palm side of the forearm
- The deep fibres of Brachioradialis
- The deep extensors of the wrist and fingers which lie on the back of the forearm
- The deep and superficial palm and finger flexors in the hand
All of these areas must be examined thoroughly for any hypertonus (tension) and deficient ranges of movement where the joints are involved.
The trained hand will know precisely where these areas are and then with the right skills, 'undo' them. The skills needed are primarily the educated sense of touch, like a potter or pianist, and then the techniques to do something about what you find.
The most commonly involved trigger areas are in the deep extensors and flexors of the wrist and fingers as well as the muscles of the Thenar eminence (thumb). This is most evident in cases where the use of a mouse and typing have over-tightened the deep extensor tendons, the deep flexor tendons and the thumb muscles. These, in order of appearance constitute the basic building block of RSI of the forearm and hands.
When you add in the all too common shoulder and neck tension patterns, you will become very likely to suffer from RSI.
What is RSI?>> RSI muscle triggers>> RSI nerve triggers>> RSI pathophysiology>> RSI treatment >>Musicians>>Myths>>Inspiration
RSI nerve involvement
If there is a tendency for nerve compression, especially involving the Median nerve, there are specific points where nerve compression can occur, They are as follows:
- Lower cervical lesions- can affect any nerve, Radial, Ulnar but principally the Median nerve. Symptoms of pain (Radial nerve) and numbness in hands. The Ulnar nerve will produce pins and needles and numbness of the outside of the hand, little and ring fingers and side of palm. Such lesions when severe produce symptoms which are constant
- 1st, 2nd and 3rd rib lesions- elevates and compresses the Brachial plexus. Principally affects the Median nerve. Not usually painful producing pins and needles and occasional numbness in the palm side of the thumb, index fingertip, middle fingertip and sometimes the tip of the ring finger
- Brachialis in the 'crook of the elbow' can further compress the Median nerve. A sign of Brachialis hypertonus is an inability or difficulty in straightening the arm at the elbow. This gives the three finger tip pattern of Median nerve symptoms
- Palmaris Longus when hypertonic pulls its fanlike attachments to the palm in will induce Median nerve compression, often in only the index and middle fingers
- The thumb muscles will produce compression principally of the Median nerve supply to the thumb
- The tendons and muscles of the index finger and thumb which produce 'pincer' type movements, when hypertonic, make numbness in the thumb and index fingers more likely
The thing to realise with trigger areas is that every point of compression you have adds to the tendency to produce both musculo-skeletal pain and pins and needles/numbness. It works like an 'amplifying' process. Each sections' tension pattern adding to its neighbours' along the same nerve pathway. It is a process of attenuation of the nerve signaling, whereby the entire nerve becomes more excitable, thus making subliminal pain spring into consciousness manifesting as a symptom. This overall excitability affects the excitibility of the reflexes and thereby the tone of the muscles involved in the highest activity rate rises and tension mounts. You know how it is when someone presses your shoulders and finds places of tension that you didn't realise were there. These areas of hypertonicity are generally not needed by the body, unless you are a lumberjack!! The point being that we are all on the verge of being in pain all the time in many places of our body its just that our nervous system cleverly 'damps' it down so that we don't suffer too much.
What is RSI?>> RSI muscle triggers>> RSI nerve triggers>> RSI pathophysiology>> RSI treatment >>Musicians>>Myths>>Inspiration
RSI Pathophysiology
I too have suffered many repetitive strain injuries as a result of the hands-on work that I do in clinic. Intense guitar playing and ‘mousing’ my PC for hours creating websites such as this one don’t help either. However, such episodes have served to edify me with regard to the general and specific nature of finger, wrist, arm, shoulder, neck and upper ribcage interactions. Said interactions manifest via lines of tension, nerve pain, pins and needles, muscle ache and joint ache by virtue of a sequence of shortening of adjacent structures in response to habit and irritation.
I have found that the majority of symptoms arise from the deep muscles, however, often the tendons of the superficial muscles are irritated as they pass over areas where the carpal bones, for example, are misaligned and or inflammed.
When the deep ‘stabilising’ muscles of the forearm become hypertonic or overly tense they lose Oxygen and rapidly tire, causing pain. This reaction in the deep muscles is more likely than with the superficial layers due to the type of reflex tone setting mechanism and because of restriction to their expansion. The girth of the deep muscles is more tightly constrained than the superficial muscles. This physical constraint to expansion is due to the membranous sheath which envelopes every skeletal muscle of the body. Described as a 'stout' membrane, the epimysium is a layer of connective tissue which ensheaths the entire muscle. It is composed of dense connective tissue and is continuous with the fascia of adjacent muscles and the internal connective tissue wrappings within the muscles.
The density of this sheath varies from deep to superficial muscle layers. Thus, when the deep muscles expand through constant and also unique occasions of overuse they become constrained by the limits of the dense membranes enveloping them. When this state of hypertonus has persisted for some time the nervous system registers the increased tone as normal and automatically maintains the tension even though it is no longer appropriate. Pain will be generally perceived at the anchor points of the muscles and their tendons i.e. the elbow and upper forearm, and the fingers and wrist.
Often I have observed that the superficial layer is weak and flaccid whilst the deep layers are very dense and shortened. Observation of top professional pianists demonstrates that the relaxed, flowing approach to playing, honed by many years of skill acquisition and the relative absence of poor postural and technique habits plus familiarity with their own repertoire serves to maximise their performance abilities. However, even these performers can be struck down by injuries such as falls on to the hand, gardening, decorating, writing, carrying heavy bags, and a host of other trauma.
The Carpal bones form a cute little paired arch which sit, tightly bound together. They can suffer from what might best be described as 'disruption'. Some of the Carpal bones can slip slightly out of line with its' neighbours. Adhesions which make the Carpal bones glue together are common, usually as the result of a fall or twist strain. The Carpals which are stuck will no longer function in their required movement ranges. These 'disruptions' are frequently painful. The type of pain can be sudden, the type that makes you whince and then it is suddenly much less when you move your hand to instinctively relieve it. These can be inflammed in very specific areas and very persistent unless corrected by accurate joint articulation and manipulation.
What is RSI?>> RSI muscle triggers>> RSI nerve triggers>> RSI pathophysiology>> RSI treatment >>Musicians>>Myths>>Inspiration
Diagnosis and treatment of RSI
The experienced hand sees by touch, the shapes, densities, heat, textures, resistances of the body, the trained mind puts it all together. The trained hand stretches and softens the specific muscles, tendons and joints as mentioned above, the experienced mind asks questions pertinent to usage and the particular trigger area under investigation. These can reveal additional information about any other activities that the RSI suffer is engaging in which might be adding an additional trigger area.
I am able, by virtue of specialised and unique hands-on techniques that I call ‘Myo-articulation’, to reverse deep tension patterns quite swiftly. If there is carpal bone derangement present, I can very specifically locate and ‘undo’ adhesions and re-align these delicate little bones of the wrist. I will ‘track’ the tension patterns along the arm and identify shoulder, ribcage and neck involvement. These I will then release using a variety of techniques such as articulation, massage and manipulation where necessary.
It is even possible to identify, by palpating the tensions in individual muscles, specific playing related patterns of overuse such as the little finger in trills on the violin, over- gripping and over-flexing in the bowing hand and much more.
Whilst 'weakness' in the muscles' is much ballyhooed, it is more usually the best procedure to save strengthening exercises until the last, once the deep muscles and joint problems have been corrected. The action of correcting a muscle will induce muscle growth anyway. It is often wise to tone up the secondary muscles involved in a given action. Typing, for example, has the Deltoid muscles as secondary stabilisers holding the arms slightly out from the body. If you strengthen these muscles the arm will feel lighter. If the Deltoids are too underused then the deep primary stabiliser, Supraspinatus will become hypertonic and will constitute another trigger area.
When I began many years ago, I took it all for granted. Having been brought up as a boy in an Osteopathic environment I didn't realise that there were many things that people didn't know about in connection with the workings of the body and what makes them function that I took for granted. Hence, trying to take the thorny subject of RSI and shake some common sense into it for you.
Sure, there are other factors potentially involved. Psychological elements, metabolic factors, ergonomic, posture, hydration levels, diabetes, hypoxia, hypercalcemia, even pollution levels, but here I have restricted my talk with you to those things that seem to be least understood by sufferers. I hope it helps you to understand more deeply the whole painful subject of RSI.
What is RSI?>> RSI muscle triggers>> RSI nerve triggers>> RSI pathophysiology>> RSI treatment >>Musicians>>Myths>>Inspiration
For Musicians
Repetitive Strain Injuries affect the spine and lower limbs as well as the forearms.
Why do some people get RSI from a particular activity whilst others performing the same activity are seemingly immune?
It would appear that the main factors in giving an increased likelihood for RSI fall into the following categories:
- Musculo-skeletal
- Nerve encroachment and compression
- Amount of time spent performing activities
- Intensity of actions required
- Fast twitch/slow twitch muscle typology
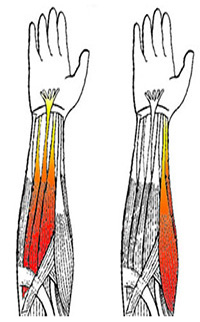
The RSI maps
As a result of many years of observation of RSI patterns of pain Paul Manley produced the ‘RSI maps’. These maps indicate the specific areas most likely to be afflicted. They enable us to interpret the areas involved and the related hand/wrist/finger/bodily functions specific to those areas. This then enables us to make recommendations regarding habits and to evaluate the nature and severity of the condition.What is RSI - Repetitive Strain Injury?
WRULD or Work Related Upper Limb Disorders is a term coined by the TUC (the British Trades Union Council) meaning repetitive strain induced by one's employment. This term includes conditions such as 'beat hand', 'white finger syndrome' and various other work related syndromes.
The principle is simple. For example if I were to stroke my cats' chin with my index finger once, there would be no problem, but if I were to do this one thousand times in an hour, both my index finger tendons and my cat would complain bitterly. The muscles and tendons effecting the movement would become tired and begin to ache. They should recover soon. But if I were then to perform the same activity each day for a week, I would probably find that I could only repeat it a few times before my muscles would feel tired and achy, plus, my cat, now with a bald chin would not be pleased.
Thus, any action repeated too many times, no matter how light, will produce a repetitive strain. 'Nintendo and Blackberry thumb' are classic examples.
RSI trigger areas : Neural
If there is a tendency for nerve compression, especially involving the Median nerve, there are specific points where nerve compression can occur, They are as follows:
- Lower cervical lesions- can affect any nerve, Radial, Ulnar but principally the Median nerve. Symptoms of pain (Radial nerve) and numbness in hands. The Ulnar nerve will produce pins and needles and numbness of the outside of the hand, little and ring fingers and side of palm. Such lesions when severe produce symptoms which are constant
- 1st, 2nd and 3rd rib lesions- elevates and compresses the Brachial plexus. Principally affects the Median nerve. Not usually painful producing pins and needles and occasional numbness in the palm side of the thumb, index fingertip, middle fingertip and sometimes the tip of the ring finger
- Brachialis in the 'crook of the elbow' can further compress the Median nerve. A sign of Brachialis hypertonus is an inability or difficulty in straightening the arm at the elbow. This gives the three finger tip pattern of Median nerve symptoms
- Palmaris Longus when hypertonic pulls its fanlike attachments to the palm in will induce Median nerve compression, often in only the index and middle fingers
- The thumb muscles will produce compression principally of the Median nerve supply to the thumb
- The tendons and muscles of the index finger and thumb which produce 'pincer' type movements, when hypertonic, make numbness in the thumb and index fingers more likely
The thing to realise with trigger areas is that every point of compression you have adds to the tendency to produce both musculo-skeletal pain and pins and needles/numbness. It works like an 'amplifying' process. Each sections' tension pattern adding to its neighbours' along the same nerve pathway. It is a process of attenuation of the nerve signalling, whereby the entire nerve becomes more excitable, thus making subliminal pain spring into consciousness manifesting as a symptom. This overall excitability affects the excitability of the reflexes and thereby the tone of the muscles involved in the highest activity rises and tension mounts. You know how it is when someone presses your shoulders and finds places of tension that you didn't realise were there. These areas of hypertonicity are generally not needed by the body, unless you are a lumberjack!! The point being that we are all on the verge of being in pain all the time in many places of our body its just that our nervous system cleverly 'damps' it down so that we don't suffer too much.
What is RSI?>> RSI muscle triggers>> RSI nerve triggers>> RSI pathophysiology>> RSI treatment >>Musicians>>Myths>>Inspiration
Myths
Focal Dystonia
(Abridged from the Dystonia association website)Professional musicians are susceptible to a number of occupational conditions, including task-specific focal dystonia.
The term focal indicates that the dystonia affects a single, specific area of the body.
The term task-specific indicates that the symptoms only occur when the individual is completing a particular task, such as playing a musical instrument.
Experts estimate that 1-2% of professional musicians are affected by dystonia, but there are likely large numbers of musicians living with symptoms who remain unidentified. Almost all individuals with musician’s dystonia are classically trained, and most are male.
The first signs of musician’s dystonia are lapses in the usually instinctive ability to perform on the instrument. Musicians may perceive the early symptoms of dystonia as a result of faulty technique or insufficient preparation. Musician’s dystonia is triggered by playing the instrument and does not typically affect other activities.
The top three musical instruments associated with musician’s dystonia are piano, guitar, and brass instruments.
Pianists typically develop symptoms in the right hand, often affecting the fingers. String players usually experience symptoms in the left hand. Guitarists and percussionists may develop symptoms in either hand. Woodwind players may develop symptoms in the hands, face, or mouth. Brass players are usually affected in the corners of the mouth and jaw.
There is typically no pain associated with musician’s dystonia.
Because musician’s dystonia is a neurological disorder, the aim of treatment is to help the nervous system relearn the ability to complete specific movement tasks without triggering dystonia.
The origins of musician’s dystonia are being researched by scientists around the world.
Hand dystonia is seen in pianists, string players, guitarists, percussionists, and woodwind players. Symptoms of hand dystonia may include subtle loss of control in fast passages, lack of precision, curling of the fingers, fingers “sticking” to keys, involuntary flexion of the thumb in strings, and tremor.
My view
There are a million subtleties involved in playing an instrument. Sometimes we lose that 'edge' that crispness, the speed. This ruins what we are playing. The audience may not perceive much wrong, but we do most definitely.We must warm up, build up the speed and strengths required each time we play our instrument. When the forearm and hand muscles are tired and tense they run out of steam very quickly. This produces aching, loss of speed and accuracy. However, when such tensions are not sufficent to trigger aching they will still affect the finer hand tasks. A scale once played rapidly can now only be played at 3/4 speed because one fingertip is not behaving itself by curling in to the palm or not moving sideways properly. So, we repeat the practice until we have regained speed and accuracy. This can take a few minutes. But when it takes hours or never re-appears as a skill we will panic. Our life is music. The first place to look is in the forearm and hand muscles. Check for dense/tense muscles and if present stretch and massage them.
With true focal dystonia the problem persists and can be due to cerebellar involvement. This part of the brain controls co-ordination. It is very vulnerable to damage from alcohol and nicotine, cells can die and with them go our abilities. All to often the diagnosis of Focal Dystonia is not appropriate without first assessing the tension patterns in the areas named above. This can only be done by a specialist due to the fundamentally tactile nature of such an examination. Mere words cannot constitute a good diagnosis. I have found that working specifically on the muscles involved results in great improvement.
Hypermobility syndrome/ Ehlers-Danlos syndromes
(Abridged from the NHS website)Hypermobile EDS (hEDS) is often thought to be the same as or very similar to another condition called joint hypermobility syndrome.
People with hEDS may have:
joint hypermobility
loose, unstable joints that dislocate easily
joint pain and clicking joints
Currently, there are no tests to confirm whether someone has hEDS. The diagnosis is made based on a person's medical history and a physical examination.
My view
A lot of physical therapists seem to love to condemn a person's condition by labelling them as hypermobile. This is ignorant and an example of lazy thinking and minimal experience in actually helping people. It is a dismissive term. The reality is quite the opposite. Most conditions related to muscles and joints are due to hypo-mobility in other words lack of mobility. It seems that many therapists don't know the difference and they have also been partially brainwashed. My Mother was a contortionist and never suffered from problems due to her hypermobility. She lived until 90. I too am hypermobile, bendy. When I fell down the stairs three years ago and ripped the hell out of my right knee which twisted up behind me, my hypermobility saved me. I ended up with a moderate avulsion fracture which rapidly healed under my efforts. So do not be fobbed off with a hypermobility diagnosis.Polymyalgia rheumatica
(Abridged from the NHS website)Meaning: Many muscle pain and joint ache
A condition that causes pain, stiffness and inflammation in the muscles around the shoulders, neck and hips.
The main symptom is muscle stiffness in the morning that lasts longer than 45 minutes. It may also cause other symptoms, including:
extreme tiredness
loss of appetite
weight loss
depression
My view
The definition of this pseudo-disorder is so vague from the NHS as to apply to the majority of the adult population. As such it is a useless diagnosis, little more than something to fill in on a form to be passed on to some other 'expert' in the field. A rheumatologist will then supply their experimental drugs and some physio. It is a helpful as a mechanic telling you that there is something wrong with your car which may or may not get better. A true mechanic looks at the structure and functions of the body and applies physical, hands-on treatment to the affected areas.Fibromyalgia
(Abridged from the NHS website)Fibromyalgia, also called fibromyalgia syndrome (FMS), is a long-term condition that causes pain all over the body.
As well as widespread pain, people with fibromyalgia may also have:
increased sensitivity to pain
fatigue (extreme tiredness)
muscle stiffness
difficulty sleeping
Anyone can develop fibromyalgia, although it affects around 7 times as many women as men. The condition typically develops between the ages of 30 and 50, but can occur in people of any age, including children and the elderly. It's not clear exactly how many people are affected by fibromyalgia, although research has suggested it could be a relatively common condition. Some estimates suggest nearly 1 in 20 people may be affected by fibromyalgia to some degree.
One of the main reasons it's not clear how many people are affected is because fibromyalgia can be a difficult condition to diagnose.
There's no specific test for the condition, and the symptoms can be similar to a number of other conditions.
My view
This is another 'rubbish bin' diagnosis into which a patient is placed in the abscence of any other diagnosis. Each patient must be physically and competently assessed especailly when they are a musician.Psychology
An interesting article on the musicians brain development.Almost 60% of professional musicians have suffered from a psychological issue and almost half have experienced problems with alcohol, according to a survey by Help Musicians UK. Focused on health and wellbeing, the research finds that anti-social working hours are the biggest concern for musicians, and speculates that this could lead to the psychological issues, loneliness and relationship difficulties that the majority of musicians report suffering from.
My view
A lot of patients that have been passed through the usual system may have had counselling and CBT which tells them to accept the problem and it will fade away. In the prescence of actual physical causes such advice can be abhorrent. If I sprain my ankle it does not help to be told to get used to it! I need help, a proper diagnosis, some way of helping myself. The first stop on any diagnosis is the proper examination of the structures involved and the associated functions and their possible over-use.Conclusion:
I have frequently helped patients out of pain when they have been given these flimsy, generalised diagnoses by professionals who don't know any better. Look at the nuts and bolts before you write-off people without first having established physical evidence.Legends
Some brave souls who persisted to greatness
Glenn Gould
Gould suffered many pains and ailments, though he was something of a hypochondriac (admitting it himself on at least one occasion), and his autopsy revealed few underlying problems in areas that often troubled him. He was highly concerned about his health throughout his life, worrying about everything from high blood pressure (which in his later years he recorded in diary form) to the safety of his hands. (Gould rarely shook hands with anyone and usually wore gloves).As mentioned above, early in his life Gould had suffered a spine injury. His physicians prescribed, usually independently, an assortment of analgesics, anxiolytics, and other drugs. Gould's increasing use of a variety of prescription medicines over his career may have had a deleterious effect on his health. It reached the stage that "he was taking pills to counteract the side effects of other pills, creating a cycle of dependency". It has been stated that Gould took a lot of antidepressant medication, which was blamed for his deteriorating mental state.
The astounding story of Glenn Gould pdf.
The Goldberg Variations (note the dreadful posture).
Jaqueline Du Pre
In 1971, du Pré's playing declined as she began to lose sensitivity in her fingers and other parts of her body. She was diagnosed with multiple sclerosis in October 1973. Her last recording, of sonatas by Chopin and Franck (the latter originally for violin), was made in December 1971. She went on sabbatical from 1971 to 1972, and performed only rarely. She started performing again in 1973, but by then her condition had become severe. For her January tour of North America, some of the less-than-complimentary reviews were an indication that her condition had worsened except for brief moments when her playing was without noticeable problems. Her last London concerts were in February 1973, including the Elgar Concerto with Zubin Mehta and the New Philharmonia Orchestra.Multiple sclerosis and Elgar, amazingly beautiful.
Itzak Perlman
Perlman first became interested in the violin after hearing a classical music performance on the radio. At the age of three, he was denied admission to the Shulamit Conservatory for being too small to hold a violin. He instead taught himself how to play the instrument using a toy fiddle until he was old enough to study with Rivka Goldgart at the Shulamit Conservatory and at the Academy of Music in Tel Aviv, where he gave his first recital at age 10. He moved to the United States to study at the Juilliard School with the violin pedagogue Ivan Galamian and his assistant Dorothy DeLay.Perlman contracted polio at age four and has walked using leg braces and crutches since then and plays the violin while seated.
Django Rheinhardt
"Before he had a chance to start with the band, however, he nearly lost his life when the caravan he and his wife lived in caught fire when he knocked over a candle on his way to bed. His wife made artificial flowers from extremely flammable celluloid. They caught fire, engulfing the wagon in flames almost immediately. Reinhardt dragged himself and his wife through the fire to safety, but suffered extensive burns on his left hand and other areas. He received first- and second-degree burns over half his body. His right leg was paralyzed, and the fourth and fifth fingers of his left hand were badly burned. Doctors believed that he would never play guitar again, and they intended to amputate one of his legs. Reinhardt refused to have the surgery and left the hospital after a short time; he was able to walk within a year with the aid of a cane.Two of his fingers remained paralyzed. By sheer will, he taught himself to overcome his now permanent handicap by using only his thumb and two fingers. His brother, Joseph Reinhardt, also an accomplished guitarist, bought Reinhardt a new guitar. With rehabilitation and practice, he re-learned his craft in a completely new way. He played all his guitar solos with only the index and middle fingers and used the two injured fingers only for chord work."
Rare footage of this amazing musician